65 yr female with head ache and and involuntary movements of limbs
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputsThis e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
65 year old female who is an agricultural labourer by occupation came with the C/O involuntary movements, giddiness and memory loss since 4 month s
History of present illness:
Patient was apparently asymptomatic 4 months back
she had H/O Fever - associated with generalised weakness which lasted for 3 days for which she visited the hospital, fever evaluation was done (dengue ,MP, Widal Negative) and
she was prescribed antipyretics for 5 days and the fever subsided within 3 days after medication
After 1 week of fever history, she had right leg pain with tingling sensation of right upper limb and lower limb (upper limb more than lower limb)- associated with sudden outstretching movements of right upper limb associated with tapping of right
These involuntary movements were episodic with a frequency of 1 episode per hour, with each episode lasting for 1-2 secs.
Movements were present at rest.
These movements were associated with giddiness.
The movements disappeared on sleeping.
Patient went to the orthopedician for her right leg pain and X-Ray was done which was found to be NORMAL after which she was referred to a neurologist where CT Brain was done which showed OLD CALCIFIED GRANULOMA
The neurologist had started her on:
Tab. Valpraote 300 mg BD
Tab. Gabapin 100 mg OD
Tab. Vitamin D3 PO/OD for 10 days
Tab. Zapiz 0.5 mg PO/HS.
the frequency of involuntary movements had decreased.
History of past illness:
Patient had a H/O head injury 20 yrs back,where she was hit with a wooden log on her head as well fall due to giddiness and she sustained an injury to her head
over the left parietal region and a bleeding happened for which she visited a local rmp doctor -- suturing was done and patient was put on antibiotic.
Because of disturbed sleep, she visited a doctor n was referred to psychiatrist and she was started on Tab. Escitalopram and clonazepam.
Personal History-
Diet: mixed
Reduced appetite.
Sleep: decreased since 10 days
Bowel and bladder habits: regular
History of tobacco chewing.
Family History:
No significant history.
General Examination:
Patient is Conscious, coherent, cooperative
Mild pallor +
No icterus/ cyanosis/ clubbing/koilonychia/ lymphadenopathy/ edema
Dry scaly skin


Vitals at admission:
Temp.- Afebrile
BP- 130/80
PR- 69 bpm
RR- 17 cpm
SpO2- 99%
Systemic Examination:
CVS- S1S2 heard, no murmurs
P/A- Soft, Non-tender
CNS-
Pt. is C/C/C
Oriented to time, place, person
Speech: Normal
Motor system: Normal
Sensory system: Normal
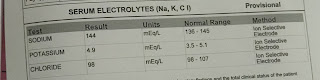
Clinical report s/investigation s









Gall bladder- distended.
Right n left kidney: decrease in size and increase in echo.
U.bladder distended- minimally.
PROVISIONAL DIAGNOSIS:
hemiballismus with dementia under evaluation
ONGOING TREATMENT:
1. Tab. Queitapine 25 mg PO/OD
2. Tab. Valproate 300 mg PO/OD
3. Tab. VERTIN 16 mg PO/OD
4. Tab. Esihans Plus(Escitalopram(10 mg) and Clonazepam(0.5 mg)) for 15 days



Comments
Post a Comment